🥦 Nutrition & Nutrients
Minerals
Research
November 26, 2025
Share

Key Physiological Functions of Magnesium
Energy metabolism and mitochondria
Magnesium is required at every stage of energy production, from glycolysis to the electron transport chain. Mitochondrial enzymes depend on magnesium to synthesise Mg-ATP.
ATP (adenosine triphosphate) is the universal energy molecule used by all cells.
However — ATP is not biologically active by itself.
For ATP to be usable, it must bind to magnesium.
This creates:
Mg-ATP — the functional form of cellular energy.
Magnesium stabilises ATP and enables enzymes to access and transfer its energy.
If magnesium is insufficient:
ATP production slows,
and the ATP that is produced cannot be effectively used.
This is why magnesium deficiency often presents as low energy, brain fog, sluggish metabolism, and increased fatigue even when sleep and nutrition are adequate.
Magnesium doesn’t just support energy production — it unlocks energy availability.
Glucose regulation and insulin sensitivity
Magnesium supports insulin receptor activity and assists glucose transport into cells. Suboptimal magnesium contributes to insulin resistance, unstable blood sugar, and cravings for carbohydrates.
Nervous system regulation
Magnesium balances brain excitability by:
reducing excessive stimulation (NMDA receptor regulation),
enhancing calming neurotransmission (GABA signalling).
This is why magnesium is clinically relevant in anxiety, sleep dysregulation, and stress physiology.
Muscle and cardiovascular function
Calcium initiates contraction; magnesium enables relaxation.
Magnesium regulates heart rhythm, vascular tone, and blood pressure.
Bone mineralisation and vitamin D activation
Magnesium activates vitamin D and regulates parathyroid hormone, directing calcium into bone tissue rather than soft tissues.
Why Magnesium-containing Foods Are Green
Magnesium sits at the centre of the chlorophyll molecule — the pigment that makes plants green.
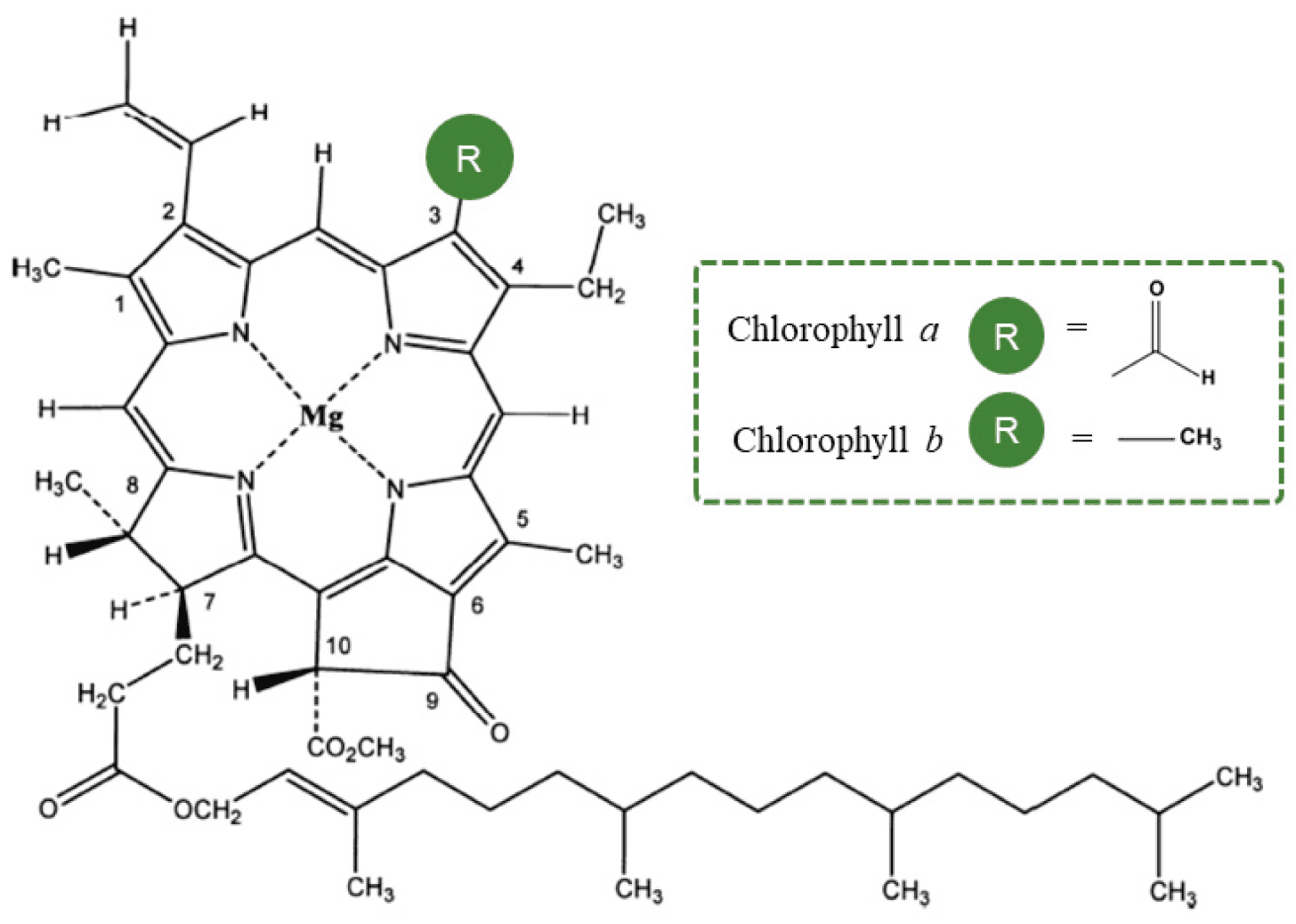
Green colour = chlorophyll
Chlorophyll = magnesium at its core
The darker the green, the higher the chlorophyll, and therefore the higher the magnesium.
Examples: spinach, kale, chard, parsley, sea vegetables.
Signs of suboptimal magnesium status
Persistent fatigue or low stamina
Muscle cramps or twitching
Restlessness or difficulty “switching off” mentally
Sugar/carbohydrate cravings
Headaches or migraines
Constipation
These reflect impaired ATP utilisation, neuromuscular irritability, and poor glucose metabolism.
Supplemental magnesium: Forms and their applications
Different magnesium compounds vary in bioavailability and tissue preference. Selecting the form based on physiological need improves effectiveness.
Form | Primary OTC uses | Typical adult dose (elemental Mg/day) | Key human evidence (headline) | Bioavailability & tolerability | Notes |
|---|---|---|---|---|---|
Magnesium oxide | Constipation, antacid; sometimes used for migraine prevention | 200–400 mg (split); laxative doses much higher (as hydroxide/oxide) | Mixed; some migraine and sleep trials show benefit; poor results in mood when used alone | Low absorption; GI laxative effect common | Cheap, high elemental % per pill but not ideal for repletion |
Magnesium citrate | General repletion, migraine prevention, mild constipation | 200–400 mg (split); one-off high doses for constipation | RCTs: ↓ migraine frequency; benefits in fibromyalgia when used alone/with meds | High absorption; mild laxative at higher doses | Strong all-rounder for raising status |
Magnesium glycinate (bisglycinate) | Sleep, anxiety/stress, muscle tension; gentle long-term repletion | 200–400 mg (split) | RCTs: modest insomnia improvements; broader Mg trials support anxiety/sleep | High absorption; best GI tolerance | Good choice when citrate causes loose stools |
Magnesium malate | Muscle pain, fibromyalgia, energy support | 300–600 mg (split) | Early trials/open-label signal ↓ pain/tender points; newer low-dose Mg trials show pain/stress benefits | High absorption; low laxative risk | Malate supports Krebs cycle; solid for neuromuscular complaints |
Magnesium L-threonate | Cognition, memory, sleep architecture | ~144–200 mg (from 1.5–2 g MgT; split) | RCTs: improved memory/exec function; emerging sleep data | Good systemic; noted CNS penetration | “Brain magnesium”; lower elemental per capsule |
Magnesium chloride | General repletion, electrolyte balance; mood | 200–350 mg (split) | Open-label: improved depression/anxiety in adults within weeks | High absorption; moderate GI tolerance | Often in slow-release tabs or liquids |
Magnesium sulfate (oral) | Short-term constipation/bowel prep | Laxative doses in grams (not for daily Mg) | Effective as osmotic laxative; not for repletion | Low absorption for status; strong laxative | Reserve for GI indications, not daily Mg |
Magnesium lactate | Gentle daily repletion, sensitive GI | 200–400 mg (split) | Small human studies: effective status raise with minimal GI upset | High absorption; gentle | Common in fortified foods/tonics |
Magnesium gluconate | Gentle daily repletion, liquids/syrups | 200–400 mg (split) | Clinical use supports good absorption/tolerance | High absorption; gentle | Useful when tablets aren’t tolerated |
Magnesium aspartate | General repletion; used in some stress/energy trials | 200–400 mg (split) | Human trials (mixed indications) support good repletion | High absorption | Aspartate is mildly excitatory at very high doses |
Magnesium orotate | Cardiovascular support, athletic use | 100–400 mg (split) | Cardiac trial data (CHF) showing functional benefits | Good absorption | Costly; niche cardiac applications |
Magnesium taurate | BP/arrhythmia support, metabolic calming | 200–400 mg (split) | Human taurine + Mg data supportive; few Mg-taurate RCTs | High absorption; well-tolerated | Useful when cardio + calming desired |
Magnesium carbonate | Antacid; incidental Mg | Variable; not typical for repletion | Antacid effectiveness; limited repletion data | Moderate when gastric acid adequate | Can bloat; needs stomach acid to convert |
Magnesium hydroxide | Laxative (Milk of Magnesia), antacid | Laxative tablespoons (not daily Mg) | Effective laxative; poor for status | Low absorption; strong laxative | For short-term GI use only |
Microencapsulated Mg (e.g., MAGSHAPE™) | General repletion where GI side effects limit dosing | 200–400 mg (split) | Human data: sustained plasma Mg, fewer GI side effects vs. traditional | Good absorption; best GI comfort |
Repletion with few GI issues: citrate, glycinate, lactate, chloride
Sleep/anxiety: glycinate; threonate (brain), taurate (calming/cardiac)
Migraine: citrate (evidence-backed); some clinicians also use oxide (less ideal)
Fibromyalgia/muscle pain: malate (plus general Mg repletion)
Constipation: oxide/hydroxide/sulfate (short-term laxative use)
Cognition/memory: L-threonate
Very sensitive gut / higher dose needs: microencapsulated Mg
Dosing shown is elemental magnesium. Split dosing (AM/PM with food) improves absorption and tolerability. Adjust for renal impairment and drug interactions (separate by ≥2 hours from tetracyclines/quinolones, levothyroxine, bisphosphonates).
References:
Baaij, J.H.F. de, Hoenderop, J.G.J. and Bindels, R.J.M. (2015) ‘Magnesium in Man: Implications for Health and Disease’, Physiological Reviews [Preprint]. Available at: https://doi.org/10.1152/physrev.00012.2014.
Blancquaert, L., Vervaet, C. and Derave, W. (2019) ‘Predicting and Testing Bioavailability of Magnesium Supplements’, Nutrients, 11(7), p. 1663. Available at: https://doi.org/10.3390/nu11071663.
Boulis, M., Boulis, M. and Clauw, D. (2021) ‘Magnesium and Fibromyalgia: A Literature Review’, Journal of Primary Care & Community Health, 12, p. 21501327211038433. Available at: https://doi.org/10.1177/21501327211038433.
Castiglioni, S. et al. (2013) ‘Magnesium and Osteoporosis: Current State of Knowledge and Future Research Directions’, Nutrients, 5(8), pp. 3022–3033. Available at: https://doi.org/10.3390/nu5083022.
Cepeda, V. et al. (2025) ‘Unlocking the Power of Magnesium: A Systematic Review and Meta-Analysis Regarding Its Role in Oxidative Stress and Inflammation’, Antioxidants, 14(6), p. 740. Available at: https://doi.org/10.3390/antiox14060740.
Gröber, U., Schmidt, J. and Kisters, K. (2015) ‘Magnesium in Prevention and Therapy’, Nutrients, 7(9), pp. 8199–8226. Available at: https://doi.org/10.3390/nu7095388.
Kappeler, D. et al. (2017) ‘Higher bioavailability of magnesium citrate as compared to magnesium oxide shown by evaluation of urinary excretion and serum levels after single-dose administration in a randomized cross-over study’, BMC Nutrition, 3(1), p. 7. Available at: https://doi.org/10.1186/s40795-016-0121-3.
Liu, G. et al. (no date) ‘Efficacy and Safety of MMFS-01, a Synapse Density Enhancer, for Treating Cognitive Impairment in Older Adults: A Randomized, Double-Blind, Placebo-Controlled Trial’, Journal of Alzheimer’s Disease, 49(4), pp. 971–990. Available at: https://doi.org/10.3233/JAD-150538.
Peikert, A., Wilimzig, C. and Köhne-Volland, R. (1996) ‘Prophylaxis of migraine with oral magnesium: results from a prospective, multi-center, placebo-controlled and double-blind randomized study’, Cephalalgia: An International Journal of Headache, 16(4), pp. 257–263. Available at: https://doi.org/10.1046/j.1468-2982.1996.1604257.x.
Rawji, A. et al. (no date) ‘Examining the Effects of Supplemental Magnesium on Self-Reported Anxiety and Sleep Quality: A Systematic Review’, Cureus, 16(4), p. e59317. Available at: https://doi.org/10.7759/cureus.59317.
Taheri, M. et al. (2024) ‘Effect of magnesium oxide or citrate supplements on metabolic risk factors in kidney stone formers with idiopathic hyperoxaluria: a randomized clinical trial’, Magnesium Research, 37(1), pp. 12–21. Available at: https://doi.org/10.1684/mrh.2024.0524.
Tarleton, E.K. et al. (2017) ‘Role of magnesium supplementation in the treatment of depression: A randomized clinical trial’, PLOS ONE, 12(6), p. e0180067. Available at: https://doi.org/10.1371/journal.pone.0180067.
Veronese, N. et al. (2016) ‘Effect of magnesium supplementation on glucose metabolism in people with or at risk of diabetes: a systematic review and meta-analysis of double-blind randomized controlled trials’, European Journal of Clinical Nutrition, 70(12), pp. 1354–1359. Available at: https://doi.org/10.1038/ejcn.2016.154.
Walker, A.F. et al. (2003) ‘Mg citrate found more bioavailable than other Mg preparations in a randomised, double-blind study’, Magnesium Research, 16(3), pp. 183–191. Available at: https://pubmed.ncbi.nlm.nih.gov/14596323/.
Zhang, C. et al. (2022) ‘A Magtein®, Magnesium L-Threonate, -Based Formula Improves Brain Cognitive Functions in Healthy Chinese Adults’, Nutrients, 14(24), p. 5235. Available at: https://doi.org/10.3390/nu14245235.
Blogs and Insights